When people talk about “sustainable packaging,” they often picture quick material swaps and bold recyclability claims. But in pharmaceuticals, it’s rarely that simple.
Pharma packaging is a safety-critical system. It protects sensitive formulations, supports regulatory compliance, and helps patients take the right medicine in the right way, every time.
That’s why packaging teams are under a different kind of pressure: they are being asked to reduce environmental impact while holding the line on performance, patient safety, and supply resilience.
At Cambridge Design Partnership (CDP), we work with pharma and healthcare teams to make that trade space manageable. The goal isn’t sustainability as a side project. It’s packaging decisions that are evidence-led, patient-centered, and durable under regulatory scrutiny.
The structural tension at the heart of pharmaceutical packaging
In practice, pharmaceutical packaging exists inside tight constraints that are in place for good reason:
- Validated moisture, oxygen, and light barriers (often with narrow stability margins)
- Strict control of chemical interactions and leachables across materials, inks, adhesives, and coatings
- Tamper evidence, traceability, and serialization requirements
- Repeatable, audited manufacturing processes with controlled change management
- Global regulatory alignment, long shelf-life assurance, long qualification cycles, and post-approval variation burden
However, here is another non-negotiable that is often underweighted in sustainability conversations: patient usability.
In effect, packaging is the interface between medicine and the person using it. It must enable patients to identify the correct drug clearly, complete any necessary inspection (for example, tamper evidence, integrity, or visual checks, where relevant), and access the drug product reliably. If a sustainability change makes a pack harder to open, harder to read, or easier to confuse, it creates a risk that overwhelms the environmental benefit.
As a result, progress is rarely about a single material substitution. Sustainable outcomes come from system decisions – barrier, labeling, usability, manufacturing, logistics, and end-of-life considered together.
Why the pressure is now unavoidable
1. Regulation is becoming a market access issue.
In Europe, the PPWR (Packaging and Packaging Waste Regulation) is now the anchor regime: it entered into force in February 2025 and will apply from August 2026, with recyclability tightening through 2030 and a formal review horizon in 2035 that is explicitly relevant to certain pharma pack exemptions. Here, the key challenge is timing: regulatory clocks move faster than pharma packaging platforms can change.
2. Stakeholder expectations are rising.
At the same time, payers, providers, investors, and patients increasingly expect credible action. Packaging is visible, measurable, and easy to compare – so it’s becoming a practical test of seriousness, not a marketing footnote.
3. The business case is shifting from “nice to have” to “must manage”.
Consequently, packaging decisions now touch cost, resilience, and speed to market: material exposure, waste fees, supply fragility, and late-stage redesign risk. In most cases, getting ahead of change is usually cheaper than reacting when options are already locked.
What we see in real programs
A few patterns show up repeatedly when teams try to move from intent to execution.
The biggest wins aren’t always in the primary pack.
In many cases, primary packaging can be the hardest part of the system to change quickly. By contrast, secondary and tertiary packaging (such as cartons, leaflets, protective elements, and shipping formats) often provide faster, lower-risk opportunities – especially when you design them to reduce total material use, improve transport efficiency, and avoid formats that create sorting and recycling problems.
“Recyclable” is not the same as “safe, compliant, and used correctly.”
For pharma, the right question is usually: What is the lowest-impact design that still delivers stability, compliance, and patient usability? That framing prevents false optimization.
Late redesign is the hidden cost.
When sustainability is added after packaging architecture decisions are made, you end up negotiating against a nearly fixed design. That’s when cost and time blow out – and when risk rises.
A practical framework for executive decision-making
If you’re leading packaging strategy, the most useful step is to turn sustainability into a structured decision process rather than a series of ad hoc requests. Here’s a framework we use with teams to keep work focused and defensible.
1. Define your non-negotiables up front
- Before exploring options, align on what cannot be compromised:
- Patient safety and correct use
- Readability and differentiation (right medicine, strength, dose, expiration)
- Access and openability under real-world conditions
- Barrier performance and shelf-life confidence
- Tamper evidence and traceability requirements
- Validated manufacturing performance and supply resilience
This avoids “optimizing” a pack into something that fails in the field.
2. Establish a credible baseline, quickly
You don’t need a year-long study to find direction. A focused baseline – material flows, key pack components, manufacturing yield sensitivity, logistics assumptions, and end-of-life reality – usually reveals where the impact sits and where it doesn’t.
This is where we often apply lifecycle thinking and our Sustainability Cleansheet method: Quantify the big cost and environmental impact drivers early so you don’t spend months improving the wrong thing.
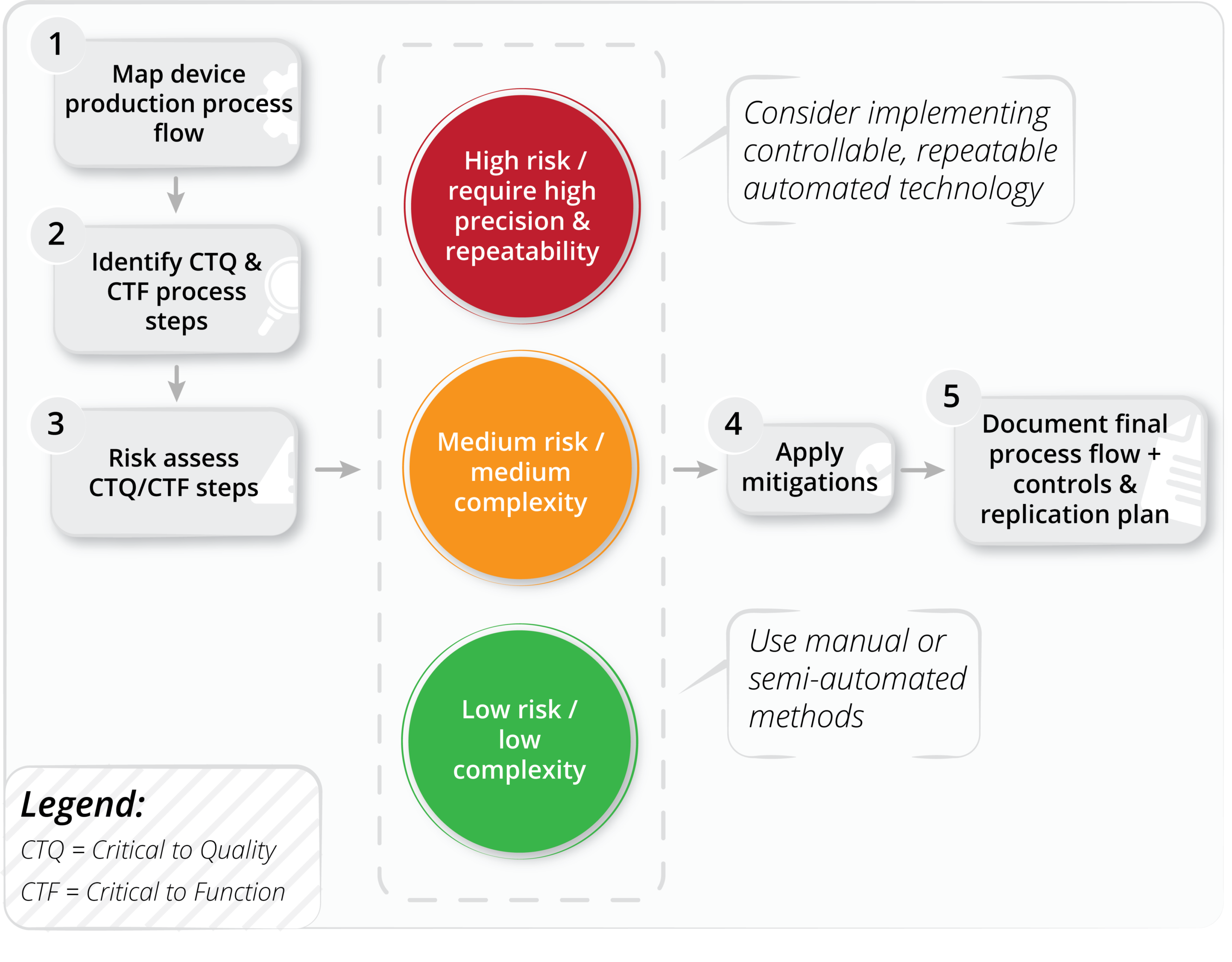
3. Build a short list of options and stress-test the tradeoffs
For each option, teams should be able to answer clearly:
- What changes physically? (materials, structure, labels, coatings, inks, adhesives)
- What risks move? (stability margin, E&L, usability, line performance, supply continuity)
- What improves? (impact reduction, cost, simplification, waste reduction, data/traceability)
- What evidence is needed? (bench tests, line trials, stability, human factors validation)
The aim is not perfect certainty. It’s the early elimination of weak options and disciplined focus on the few options that can scale.
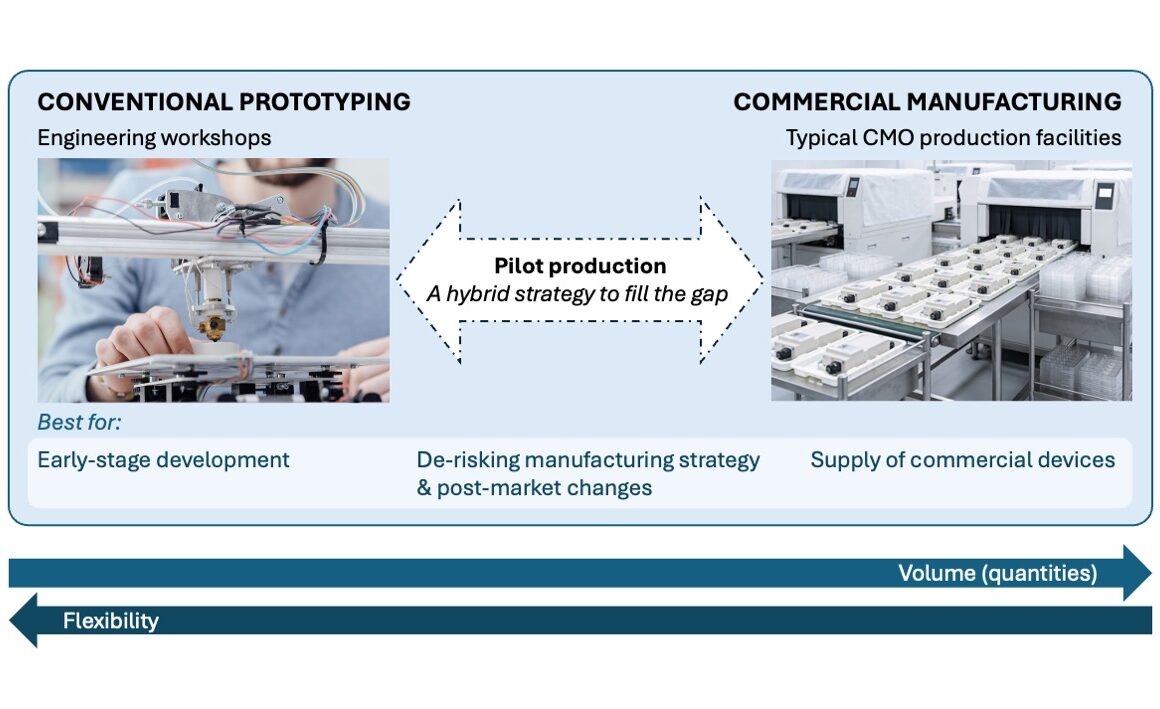
4. Pilot to reduce uncertainty, not to signal virtue
In pharma, pilots only matter if they answer hard questions: manufacturability, patient behavior, stability confidence, and real end-of-life outcomes (not just theoretical recyclability).
We design pilots to generate decision-grade evidence, so teams can commit without gambling.
5. Use “smart print” technologies thoughtfully
Many teams want digital capability – traceability, anti-counterfeit protection, patient guidance, or better sorting instructions – without turning packaging into electronics.
That’s where smart print technologies can help: Printed features (from advanced QR codes and variable data to printed conductive inks and thin printed circuits) can deliver “DPP-style” benefits – linking the pack to verified product data, instructions, and chain-of-custody information – without adding bulky components.
But they still require end-of-life thinking. Even small amounts of conductive ink or functional layers can affect recycling behavior and material recovery if they’re used indiscriminately. The practical approach is:
- Keep digital features as light as possible (often secondary packaging is the right home)
- Avoid designs that contaminate or complicate recycling streams
- Choose materials and inks with recovery pathways, where available
- Be explicit about the end-of-life intent, not just the in-use feature set
Smart features can support compliance and patient outcomes – but only if they’re designed as part of the packaging system, not bolted on.
6. Build a roadmap that matches pharma timelines
Packaging change in pharma is slow by design: qualification, validation, supplier readiness, and stability programs all take time. That’s exactly why the gap between product development cycles and regulatory timelines matters. The right roadmap staggers effort:
- Near term: Secondary and tertiary improvements and material reduction
- Mid term: Architecture changes where stability risk is manageable
- Long term: Platform shifts and primary packaging strategies aligned to the next regulatory horizon
How CDP helps
Clients bring us in when they need momentum without compromising on safety. What makes CDP different is the way we connect the disciplines that usually sit apart:
The result is packaging strategy that holds up: Lower-impact solutions that are still manufacturable, compliant, and usable – built on evidence rather than hope.
The opportunity
Sustainable pharmaceutical packaging isn’t about copying approaches from consumer goods. It’s about designing within the constraints that matter – stability, safety, usability, and supply assurance – while still making real progress on impact.
If you’re responsible for packaging strategy and you’re facing tighter timelines, rising expectations, and harder tradeoffs, we can help you move faster with confidence.