How fast can you bring new Surgical Robotics tech to market? Know the 3Cs to rapid development.
SUMMARY
- Speed to market has essential benefits for all top Robotic Assisted Surgery (RAS) companies – from maintaining and driving investor confidence to realising the commercial value as quickly as possible. But speed is often associated with risk.
- Bringing new surgical robotics development tech to market quickly and confidently requires the 3Cs: Capability, Capacity and Culture.
- A skunkworks approach provides R&D teams with all 3Cs, allowing them to focus on working without interference or interruption.
- Our RAS leadership team will be speaking at DeviceTalks Boston on April 30, on the 3Cs and showcasing an example of a successful robotic assisted surgery device design and product development for one of our clients.
Companies that build technologies for robotic-assisted surgery (RAS) are under growing pressure to deliver new products quickly. Whether you’re a global corporation or a small startup, you need to show executives and investors that you can rapidly innovate and go to market, and you need to realize the value of investment as quickly as possible. The keys to moving fast, avoiding risks and maximizing the odds of market success? Capability, Capacity and Culture.
If you’re a longtime leader in MedTech, you undoubtedly have capabilities with a large in-house talent pool of experienced engineers, design experts and other specialists. But your development efforts can stumble if teams are stretched thin across multiple projects or are delayed by bureaucratic red tape – which are problems of capacity and culture.
If you’re a startup, on the other hand, you might have launched with a promising concept but lack the breadth and depth of capabilities, and the maturity in all three Cs. Without a broad and deep field of experts – capability and capacity – and a proven culture built on the experience of delivering many other previous projects quickly, you might struggle to meet investors’ expectations of fast results.
What’s the solution to bringing all 3Cs together? A skunkworks approach.
“A skunkworks approach enables R&D teams to focus on projects in a way that’s protected from distraction, such as internal politics,” says James Boonzaier, Deputy Head of RAS and part of Cambridge Design Partnership’s new RAS leadership team. “Too often, what we see is that key people are constantly being pulled onto other projects, or they’re spread too thin, or there are political agendas getting in the way of things. In order to get these programs running fast, you need capability, capacity and culture. Capability means, ‘Do you have the required skills across your individual engineers’ brains?’ Capacity means, ‘Are they available right now?’ And culture is, ‘Are they able to work in the right kind of context for fast, deliberate progress?’”

“In order to get these programs running fast, you need capability, capacity and culture.”
James Boonzaier | Deputy Head of RAS at Cambridge Design Partnership
A Better Approach to Rapid Surgical Robotics Development & Design
Cambridge Design Partnership’s (CDP) new RAS leadership team is headed up by Tom Brittain, James Boonzaier and Jack Hornsby. Their focus on fast delivery reflects CDP’s ongoing investment and long record of success in surgical robotics
CDP strengthens its clients’ RAS programs by enhancing capability, capacity, and culture. The company’s specialists work closely with client development teams to accelerate innovation and delivery.
“Key to working this way is being able to match highly skilled and technically capable people with the right expertise, experience, personalities, and a passion for RAS, and providing them with the right tools, conditions and working environment within which to do the best possible job,” says Tom Brittain, Head of RAS. “By collaborating closely with our clients’ teams, we’re able to operate as an extension of their own pool of people. And since we’ve been active in this sector, having worked with a number of the big players in surgical robotics, we know this approach works time and time again.”
This way of working, Tom says, enables quick development by providing organizations with turnkey access to deep technical expertise, system-level thinking and user-focused design capabilities. He notes that CDP’s success in the sector relies on a team dedicated and often exclusive to surgical robotics, with bespoke teams of experts often embedding with clients according to the unique requirements of each project.
“We’re passionate about our mission and committed to helping our clients’ RAS projects succeed,” says Tom. “And our approach works, as our track record shows. Since 2019, we’ve built four complete systems, along with multiple subsystems, for clients from the ground up. These have included both blue-sky development and remedial redesign with total system architecture development. Each of these systems has been designed and manufactured in under a year, which represents extraordinary speed in this industry. We have supported several single port trans-umbilical NPD programs, with detailed engineering of capital equipment, disposables and reposables, draping systems and more. This was made possible only by having the right capabilities on site, with the right capacity available as needed, all supported by a culture of innovation.”

“Since 2019, CDP has played a substantial role in four notable product development programs in robotic-assisted surgery, delivering system-level prototypes from the ground up. Each of these has been designed and manufactured in under a year, which represents extraordinary speed in this industry.”
Tom Brittain | Head of RAS at Cambridge Design Partnership
You need a strong foundation from which to build any RAS system
The development of any RAS system requires a strong foundation of strategy and system architecture between hardware and software, all aligned to the clinical user’s needs.
James states, “To ensure strong system architecture for our clients, we really focus on conducting structured clinical needs gathering to generate solid initial hypotheses on key requirements and constraints. Once a strong foundation for the platform architecture is created, we shift our focus to the high-risk areas.”
Risk management is vital throughout the entire process. Jack calls the approach CDP takes “targeted derisking,” adding, “we know from experience what the concept killers are and what we need to do to gain confidence that we’ve solved or avoided them. That is a key element of moving quickly. Not only that, the way in which we derisk is targeted in such a way that we’re not adding more complexity or unknowns. This enables us to iterate designs quickly, learn from each step what works and what doesn’t, and develop working prototypes at speed.”
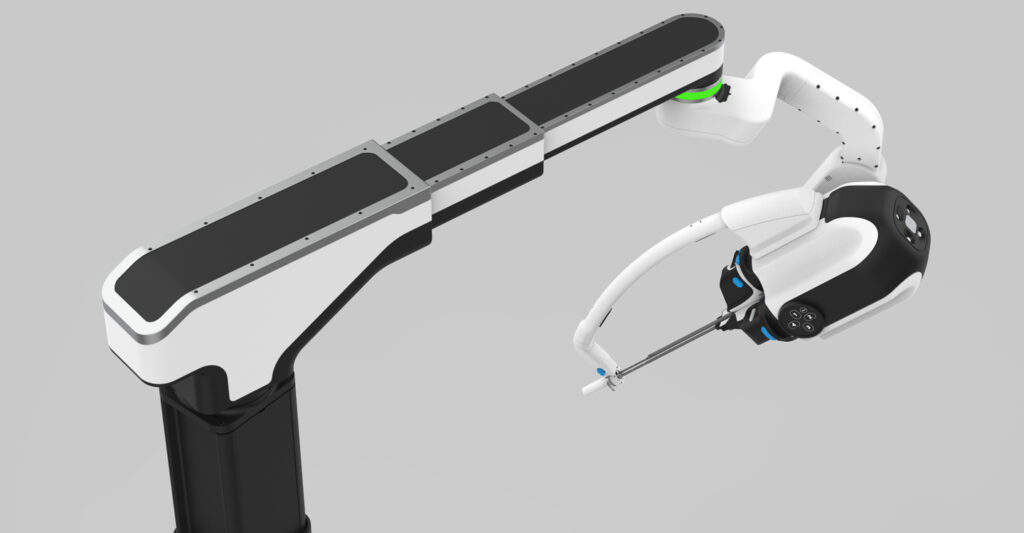
Putting this approach into practice, CDP developed a single-port RAS prototype platform, moving from an early-stage concept to an alpha system prototype for pre-clinical trials in just seven months. Jack makes the further point that “In addition to speed, the client gets to retain all knowledge and intellectual property rights for any technologies developed for them.”

“The way in which we derisk is targeted in such a way that we’re not adding more complexity or unknowns. This enables us to iterate designs quickly, learn from each step what works and what doesn’t, and develop working prototypes at speed.”
Jack Hornsby | Deputy Head of RAS at Cambridge Design Partnership
Meet the RAS Team at DeviceTalks Boston
Building a surgical robot takes true teamwork. Success demands rapid development while meeting strict clinical and regulatory requirements. Cambridge Design Partnership continues to invest in the expertise and processes that help clients bring advanced surgical robotics to market.
The result is a comprehensive offering with unmatched expertise. Clients gain immediate access to deep knowledge in kinematics, human factors, cart design, optics, systems engineering, and disposables development. And our 26,000-square-foot Pilot Production Center quickly takes a client’s project from concept to prototype build to transfer to manufacturing.
Tom, James and Jack will be speaking at DeviceTalks Boston on April 30 about the importance of the 3Cs (“How Fast Are You? Accelerating Next-Generation Surgical Robotics”). They’ll also be showcasing a platform we developed that demonstrates our approach, going from early concept to Alpha prototype for preclinical studies in under seven months. They will be on hand at stand 735 to talk about CDP’s approach to rapid development in RAS. You can also reach out in advance and chat, or book in some time to meet them in Boston.
Connect with CDP
If you would like to discuss the content of this article, please get in touch with our RAS leadership team; Tom Brittain, James Boonzaier and Jack Hornsby
Tom Brittain, Head of RAS
tom.brittain@cambridge-design.com
James Boonzaier, Deputy Head of RAS
james.boonzaier@cambridge-design.com
Jack Hornsby, Deputy Head of RAS
jack.hornsby@cambridge-design.com